Mike Paskavitz, VP of Strategy and Product, AmplifireA March 19 study in JAMA Internal Medicine reported that a Harvard-led study found that patient mortality rates drop when The Joint Commission (TJC) is physically in the hospital. This is kind of a Deus Ex Machina claim; their mere presence saves lives. But let’s explore this issue because it’s important.
Specifically, the study of 1,984 patients admitted to hospitals between 2008-2012 found that patients admitted during an unannounced Joint Commission survey had lower 30-day mortality rates than those patients admitted three weeks before or after the unannounced survey. The JAMA study’s authors said the most probable reason for the decrease in mortality during survey weeks is the “heightened scrutiny during visits” and the physical presence of surveyors, similar to how the Hawthorne effect contributes to better hand hygiene compliance. Why is this study important? At first glance, it looks like it touts The Joint Commission as the long arm of the law and that hospital staff fall in line and take the best care of patients when being off their game could get them in trouble. In other words, the fear inspired by Joint Commission surveyors brings out the best in hospital staff. Really? So what are we to do with this finding? Are we to extend greater superpowers to The Joint Commission to instil more fear, more continuously in hospital staff so that patients are safer? To do so would require a constant TJC presence in hospitals. How is that possible? More surveyors? More frequent unannounced surveyors, or 24/7 drone surveying? Deputized hospital staff to serve as whistleblowers? More real-time access to quality and safety data by TJC to monitor when things may be going wrong and swoop in with tasers? The abiding question is whether fear is a sustainable motivator for performance. This study would suggest that fear works. But if you’re like me, when I’m in a state of fear, I seek the comfort of authority, I don’t trust my own judgment, I don’t use my peripheral vision, and I get frustrated by the sense of oppression. So, the REAL question from this study isn’t how we get more Joint Commission in healthcare; it’s how do we liberate healthcare from The Joint Commission to perform well without fear. An antonym of fear is confidence. Today’s physicians and healthcare professionals have every reason to be afraid and every reason to lack confidence. Every decision made for patients is scrutinized by payers, regulators, and risk underwriters, with harsh consequences. Professional judgment is being codified into guidelines and standards of care because rogue physicians may go “off book” when caring for patients. Metrics are imposed on physicians that are supposed to represent “quality”, and performance against them is publicly reported, not to mention financial penalties levied on those whose numbers don’t measure up. In other words, doctor, we don’t trust you. But just because you are confident doesn’t mean you’re correct. Just as being correct isn’t of great value if you don’t act on it with confidence. The answer would seem to be that physicians and staff being Confident AND Correct is the best way to ensure performance. In an industry that is utterly dependent on knowledge, being Confident and Correct when making care decisions is the best alternative to an oppressive Draconian system of regulatory oversight and fear-based motivation. Prolific advances over the last 25 years in the brain science of how people learn and remember now make it possible to embed knowledge in people and commit it to long-term memory, at scale, without relying on extraordinary teachers available 24/7 or an oversight process that scares people into learning and remembering. I am not suggesting that physicians are infallible or that they know more than they do. In fact, in our work using Amplifire in healthcare so far, most physicians are confident and incorrect about 25-35% of what they need to know, and that needs to be and can be corrected. Correcting misinformation is ultimately what The Joint Commission’s job is. But the JAMA article’s suggestion that beefing up The Joint Commission’s presence in hospitals to keep staff motivated to do the right things right more often is neither scalable nor sustainable. Offering hospitals and physicians a scalable way to stay current and continuously fend off misinformation so that physicians are both confident and correct is the best pathway to improving healthcare performance. In the 1991 film called Defending Your Life, Albert Brooks plays a recently deceased man who is in a celestial weigh station where people defend the quality of their lives on earth as a way to make the case that they are worthy of advancing to the next level of existence in the universe. Brooks’ defense attorney Rip Torn explains to Brooks that, “the point of this whole thing is to keep getting smarter, to keep growing, to use as much of your brain as possible. Fear is like a giant fog, it just sits on your brain and blocks everything—real feelings, true happiness, real joy, they can’t get through that fog. But if you lift it, buddy, you’re in for the right of your life.” Mike Paskavitz, VP of Strategy and Product, Amplifire30%. $2.4 trillion. 12 minutes. 1.8 million.
What do those numbers have in common? The answer is physicians:
Technology has the potential to serve as the spine of physician alignment because of its mobility, flexibility, personalization, dynamic modality, and immediacy. Used in combination with a well thought out strategy and effective engagement methods, technology offers a cost-effective, highly-scalable way to enable effective engagement and alignment. But before you ask a physician to look at a mobile phone, download an app, read an email, open a file, attend a meeting, or change anything they’re doing, realize that there is a secret handshake among them, a password or algorithm that holds the key to getting and keeping their attention and making them open-minded to doing something differently. Call it empathy, but we’ve learned through trial-and-error that there are 10 questions that physicians ask themselves before deciding to invest their limited time and attention:
Sandy McKee, Senior Marketing Manager, AmplifireMedical errors stubbornly remain the third-leading cause of death in the U.S. Although medical institutions are investing in new patient safety training, it has not been enough to put a dent in this global problem.
Why is this and what can be done? Cognitive Learning Behavior A big part of the problem lies in the fact that traditional classroom training, while inexpensive, is only partially effective because learners will forget 75% of the material in about a week. Traditional teaching methods employ passive forms of learning, such as lectures and reading. Neuroscientists have found that humans learn more and retain information longer when active and varied learning techniques are used. When learning is made harder, knowledge sticks. (Henry Roediger, author of Make It Stick). Learning on The Job Healthcare professionals are expected to take what they have learned in the classroom and apply it on the job. While this practice is common in most professions, in healthcare, the stakes are simply too high. Healthcare professionals need a safe learning environment to practice and perfect their technique. Simulation-based training seems to be the answer. Simulation-based Training Medical simulation training has proven to be 95% effective. Meaning only 5% of the knowledge is forgotten. Simulation-based training gives medical students the opportunity to repeatedly practice a technique until they have mastered it. “Training that simulates the kinds of demands and changeable conditions that can be expected in real-world settings help learners and trainers assess mastery and focus on areas where understanding and competency need to be raised”, says Roediger. The benefits of medical simulation-based training are indisputable. In an ideal world, all healthcare providers would experience hands-on training before practicing on an actual patient. The University of Tennessee Health Science Center has invested in a new a $37 million medical simulation facility opening in the fall. It will house exam rooms, hospital beds, operating tables, residential settings, and even a pharmacy where medical students will receive hands-on training. Why aren’t more healthcare systems and medical teaching facilities quickly adopting this methodology? Look at that price tag – $37 million. Healthcare Training Needs to Be Scalable and Affordable Medical simulation facilities and programs are cost-prohibitive for many medical institutions, yet to significantly reduce medical error, an alternative training solution must be found that is:
Amplifire has developed new ways of measuring knowledge acquisition, content mastery, and retention. Amplifire’s learning management system is different from any other because it:
There is no one solution to improving patient safety. It will take a combination of training techniques and tools to solve this global healthcare problem. But a learning approach that is scalable and affordable will help healthcare systems move the needle in reducing avoidable patient harm. BY Mike Paskavitz, VP of Strategy and Product, AmplifireA Pattern We Have Never Seen: An Extraordinary Amount of Uncertainty Amplifire has measured certainty through nearly a billion learner interactions over the last decade. What we’ve never seen before is high uncertainty among clinicians. Usually, doctors are confident in what they think they know, but in our latest sepsis pilot, doctors had high levels of uncertainty regarding new information about sepsis. The sepsis course was designed around the latest evidence-based data, practices, and bundles in recognizing and treating sepsis. The doctors perceived correctly that this was new information for them and were honest about their uncertainty. Human beings are predisposed to overconfidence because it’s an adaptive feature that was forged in human psychology. Confidence is an attractive trait that has led to survival and success for those who display it proudly, even when that confidence is sometimes misplaced. It is difficult for most professionals to acknowledge their uncertainty, even when it is warranted. Not so with these docs. 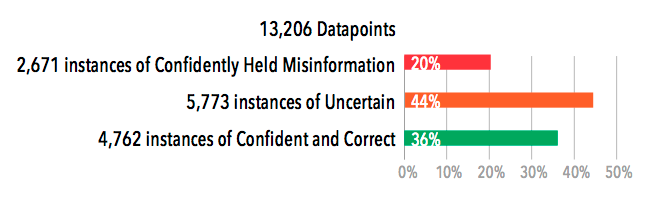 Visualizing Clinician Variation Doctors need the freedom to exercise their decision-making powers in the face of human complexity. However, doctors should not be making decisions based on out-of-date information. Old information that gets welded into memory in medical school is hard to identify and harder to eliminate. Continuing medical education has no ability to identify this confidently held misinformation (CHM), much less eliminate it. The wide range of doctor experience since medical school is what we are seeing when we look at the variation among doctors seen below. The graph shows the range of confidence and accuracy for three doctors pulled from the best, average, and worst ends of the heatmap. 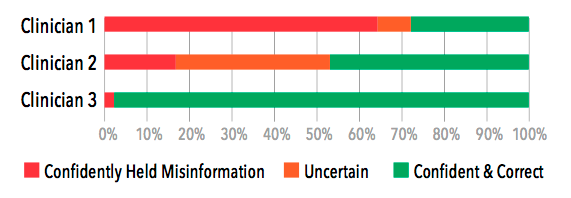 Full Results: Recognizing Sepsis Module (31 questions)  BY Mike Paskavitz, VP of Strategy and Product, Amplifire
More than anything, physicians want clarity. They want to be empowered to make evidence-based decisions that lead to the best possible patient outcomes.
When physicians scream for more evidence-based medicine, they’re really screaming for involvement. They want a say in the content of their training – will it focus on guidelines, and if so, will those guidelines align with evidence? You want to help them, but so far, your training options have been limited. You’ve found that superficial training simply doesn’t elicit enthusiasm or buy-in. Helping physicians means implementing a training program that gives them a voice. You need an evidence engine that involves physicians in the process of finding and fixing confusion. The Future of Evidence-based Medicine The Institute of Medicine said 90% of medical decisions will be based on evidence by the year 2020. This is based on the assumption that medical evidence will become increasingly available, shared, and understood. Policymakers, payers, hospitals, doctors, nurses, and patients will need to join together to rein in the evidence and use it as a weapon for harmony. Finding and Fixing Confusion We share your passion for evidence and physician involvement. That’s why we developed a method of mapping physician knowledge that doesn’t point fingers, but leads to discussion. Amplifire is an evidence-based learning platform that aims to reduce clinical variation without forcing physicians to follow protocols they don’t believe are evidence-based. Detailed learning data ensures that hospitals and healthcare systems take seriously the input and evidence from physicians, and use it to arrive at evidence-based practices embraced by all. |
PurposeThe purpose of the Medical Education Forum is to exchange thoughts, ideas, and best practices in medical education. Whether CME accredited or not, medical education is the process of facilitating learning, or the acquisition of knowledge, skills, values, beliefs, and habits. The value of medical education can not be understated but it can be under measured. The mission of this forum is to help generate new insight into the best approaches and ways to measure medical education thus empowering healthcare providers, patients and payers, to make the best choice in treatments. If you have an idea or would like to publish an article on data in this forum please send a communication through the members page, we will then review and either respond back or publish your article. Archives
July 2018
Categories |
 RSS Feed
RSS Feed
|
|
© COPYRIGHT 2018. ALL RIGHTS RESERVED.
|